Definition:
A ‘near miss’ event refers to any error which if undetected, could result in the determination of a wrong blood group or transfusion of an incorrect component, but was recognised before the transfusion took place.
A wrong blood in tube (WBIT) is defined as where blood is taken from the wrong patient and is labelled with the intended patient’s details OR blood is taken from the intended patient, but labelled with another patient’s details.
Near miss (NM) reports were first trialled in the 1997/98 Annual SHOT Report using a very small sample of hospitals over a period of a few months. In subsequent years this trial was extended to include more hospitals, until 2000/01 when all hospital were encouraged to submit NM reports. However only 29% of hospitals chose to participate at that time. The number of submitted reports and participation rates gradually increased over the next few years until data collection was halted in 2006, and the process for collecting NM reports was reviewed.
Following a new pilot study in 2009, SHOT re-started the collection and analysis of NM reports in 2010. These NM reports now account for approximately 40% of all reports submitted to SHOT. Reporting and investigating near misses can help to identify and control risks before actual harm results, providing valuable opportunities to improve transfusion safety.
More than half of the NM reports involve wrong blood in tube errors.
Recent Recommendations
Training about patient identification bands should be reviewed and their importance emphasised
Action: Education teams, hospital transfusion teams and maternity leads
In line with the HSSIB recommendations, local organisations should review and identify system-wide requirements for scanning in positive patient identification since the use of scanning technology can help to reduce misidentification incidents
Action: Hospital chief executives and medical directors
Near Miss Resources
Near Miss Webinar Wrong Blood in Tube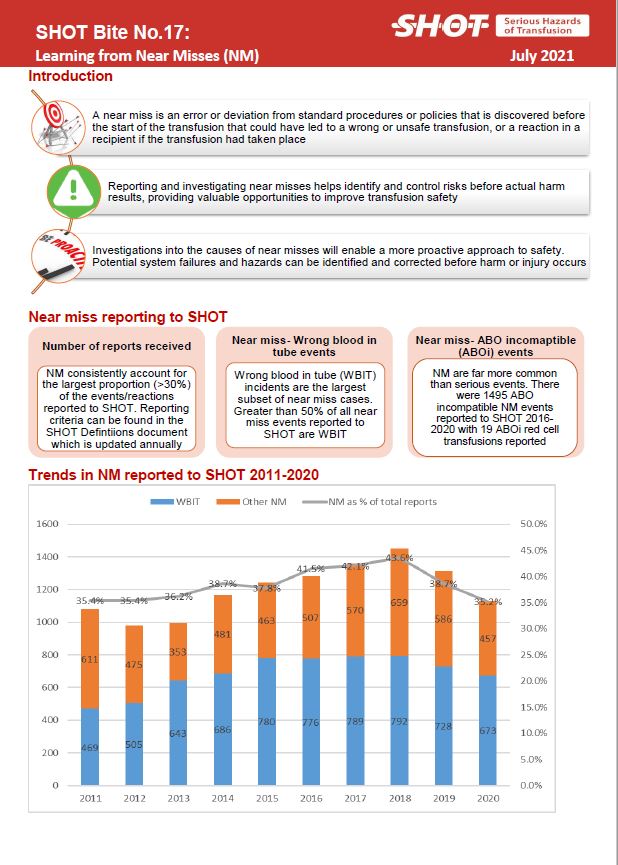
SHOT Bite No.17: Near Miss (2021)
Wrong Blood In Tube (WBIT) Investigation template
NM Annual Report Chapters
To access the chapter click either on the cover of the Annual SHOT Report or the link below the picture


















Near Miss Reporting (NM) 2001-02
Near Miss Reporting (NM) 2000-01
Near Miss Reporting (NM) 1999-00
Near Miss Reporting (NM) 1998-99
Near Miss Reporting (NM) 1997-98